

Contrast agents have been shown to be useful to improve the image quality in echocardiography. The development of new ultrasound contrast agents and imaging techniques has enabled the bedside assessment of myocardial function and perfusion.
For almost 40 years, Cardiac ultrasound has been demonstrated to be a promising diagnostic tool to evaluate patients with pericardial, valvular heart disease and patients with ischemic heart disease. However, inadequate endocardial visualisation occurs in up to 20 per cent of cases during echocardiography and it fails to produce diagnostically useful images. Contrast agents have been shown to be useful to improve the image quality (endocardial definition) in 2D and 3D echocardiography. This problem is even greater in patients referred for stress echocardiography when subjective assessment of regional wall motion is dependent on the quality of the images recorded. In stress echocardiography optimal endocardial border delineation is needed in all segments. Images are worse during stress because of cardiac movement and also hyperventilation. Although image quality has been improved with the introduction of harmonic imaging, the quality of many studies still remains inadequate. To improve the quality of images, millions of contrast agent applications have already been given to the patients since 90s.
At present, three contrast agents are licensed for left ventricular (LV) opacification and endocardial definition: SonoVue (Bracco Diagnostics Inc, US), Luminity (Lantheus Medical Imaging; trade name Definity in US) and Optison (GE Healthcare, US). The latter is currently not available. All these agents provide intensive opacification of the left heart chambers when administered intravenously. Although infusions are preferred for assessment of myocardial perfusion, bolus injections of agents may be satisfactory for left ventricular opacification in many cases. All agents are suspensions of microsheres filled with a perfluorocarbon gas and have a similar size as red blood cells. The dosages of contrast needed for LV opacification are minimal (0.1-0.3 ml) compared to those in other imaging modalities, such as X-ray for instance. These small dosages are possible because of very sensitive contrast specific imaging technologies, which have been implemented in all state-of-the-art ultrasound systems.
Ultrasound contrast agents have been licensed for improvement of endocardial border definition by left ventricular opacification. But left ventricular opacification is inevitably associated with myocardial opacification—in particular when the newer contrast specific imaging modalities are used. Assessment of myocardial opacification provides very important information on top of the evaluation of the wall motion. Questionable findings of wall motion can be clarified by assessing left ventricular opacification and vice versa.
Homogeneous myocardial and quick opacification of the myocardial vessels after LV ventricular opacification indicate normal myocardial perfusion and provide further confirmation of a normal wall motion study. This is particularly helpful in stress echocardiography. Reduced opacification in the subendocardial layers usually indicates reduced perfusion and is often easier and earlier to appreciate than a new wall motion abnormality. For rest echocardiography, the assessment of myocardial opacification is also very helpful. In an akinetic segment, lack of myocardial opacification indicates viability. Thrombi can be distinguished from tumours due its lack of opacification.
The threshold for ultrasound examinations is usually very low and the results of the examinations do not always affect the patient management. Considering the extra time, additional costs and small risk of intolerance, contrast echocardiography needs a more disciplined approach. There are a lot of patients, in whom echocardiographic images are not optimal due to factors such as obesity, lung disease, recent thoracic surgery or positive-pressure ventilation. Nevertheless, echocardiography still gives the correct answers to the clinical questions.
According to the guidelines of the American Society of Echocardiography, there is an indication for contrast echocardiography when the endocardial border definition in two or more segments is poor. In some patients poor visualisation of two myocardial segments may change management, in others Stress examinations present altogether different situation. For this kind of examination, image quality is crucial; suboptimal images of the LV cannot be accepted.
The complexity of protocol and the risks of ischaemia can only be justified if the test is diagnostic. Therefore, high image quality is vital. In these patients, contrast administration is of great importance in delineating the endocardial border in all segments, thus changing the way patient is managed. These considerations are reflected in the most recent published guidelines of European Society of Cardiology (ESC), British Society of Echocardiography (BSE) and the American Society of Echocardiography (ASE) for the clinical application of stress echocardiography. Therefore, the use of contrast agents is highest in stress echo departments—at the John Radcliffe hospital about 60 per cent of all stress echocardiograms are performed with contrast.
In the rest, contrast echocardiography is useful when minor changes of LV volumes and ejection fraction change management. Many studies have demonstrated that contrast-enhanced assessment of LV volumes and LV ejection fraction compares favourably with the accepted gold standard of cardiac magnetic resonance imaging. Monitoring of LV function during treatment with cardiotoxic drugs like Herceptin is a good example for the need of accurate assessment of LV function. In patients with poor acoustic windows, the reproducibility of contrast-enhanced studies is comparable to MRI recordings.
For ultrasound, side effects have been reported in contrast agents, but they are usually mild. However, rare allergic, potentially life-threatening reactions may occur and the investigators have to be prepared for such an event.
In April 2008, the US Food and Drug Administration (FDA) performed a safety review of the US approved perflutren microsphere contrast agents (Definity and Optison) and revised a previous black box warning. The new contraindications are much less restrictive than the previous contraindications and satisfy the needs of clinical echocardiography.
The FDA revised the benefit / risk assessment for patients with unstable conditions and acknowledged that some of the fatal events may be coincidental and not related to the contrast media. Only four fatal events with Definity occurred within 30 minutes after the application of contrast in a total of 2 million vials used.
But even if we assume that all four cases are related to the ultrasound contrast agent, the fatal event rate would be only one in 500,000 for Definity and zero for Optison. This rate is far less than the fatal event rate in exercise and Dobutamine stress echocardiography. Meanwhile, several studies were conducted on more than 20,000 patients demonstrating the safety of ultrasound contrast agents during stress echocardiography and myocardial perfusion imaging using the flash-replenishment technique.
Data collected during Post-Marketing Surveillance referred to more than 200,000 of SonoVue vials used, indicate that serious adverse events (SAE) are rare (0.01 per cent). The signs and symptoms of most of these SAEs indicate an underlying allergy-like mechanism and they were considered by the European Medicines Agency (EMEA) in the context of idiosyncratic, hypersensitivity reactions. This kind of reactions (allergy-like) is well known from wide reports in literature to occur with other medical imaging agents such as X ray or MRI contrast media.
Assessment of risk / benefit means to compare the risks of the procedure—here contrast echocardiography—with the risks of an incorrect diagnosis when not using the contrast agent. If, for instance, a new wall motion abnormality is not detected in stress echocardiogram because the wall is not adequately imaged, the diagnosis may be inaccurate and subsequent management of the patient may be wrong. Although it appears to be very convincing that patients with a missed diagnosis of coronary artery disease have an unfavourable outcome, there is only limited data to quantify the extent to which this might happen.
It appears to be easier to assess the risk / benefit when we consider false positive studies. Usually coronary angiography is requested in the case of a false positive stress echocardiogram. This will expose the patient to significant radiation and there is a procedural risk, which certainly exceeds the risk of an adverse event when using an ultrasound contrast agent.
Therefore, it is very important to take a decision whether to continue in a study, which has suboptimal images or do other kind of choice considering all the possibilities in the context of ensuring to the patient the most adequate medical treatment. Even when the risk of serious adverse events is very low, there should be a clear benefit from the application of the contrast agent to justify its use. In patients undergoing stress echocardiography, the benefit of using a contrast agent certainly overweighs the small risks—in particular when the current contraindications are not ignored.
Contrast echo closes the gap between native echo and cardiac MRI in patients with poor acoustic windows.
Harmonic imaging has been developed primarily as a contrast specific imaging modality that can be used with a transmit power (mechanical index <0.6) lower than that used for non-contrast imaging (mechanical index >1.0). Harmonic imaging has become the standard imaging technique for native echocardiography. For clinical contrast echocardiographic studies, the contrast specific imaging modalities should be used (see next paragraph). Harmonic imaging may be used only if they are not available. In order to use it for contrast studies one has to reduce the transmit power. However, the transmit power is still relatively high and can cause destruction of the contrast in the near field of the transducer as well as tissue signals of the myocardium, which impair the delineation of the endocardium.
Latest developments, such as Power Modulation and Power Pulse Inversion, which use very low non-destructive transmit power techniques (mechanical index <0.2), allow for real-time imaging without the limitations of harmonic imaging. As tissue returns are not displayed, unlike with high powered techniques, they are ideal for accurately delineating the left ventricular borders. Low power-contrast specific techniques display the contrast within the cavities and the myocardial blood within the intra-myocardial vessels. The blood volume within the myocardial vessels makes up only 7 per cent of the myocardial tissue. Therefore, the myocardial opacification is always much less intensive than the cavity opacification and provides an excellent contrast for endocardial delineation (Figure 1). The myocardial contrast is also very useful for assessing thickening of the myocardium and myocardial perfusion. Whenever available, low power contrast specific imaging techniques should be the first choice. These contrast specific imaging modalities are available in all state-of-the-art ultrasound machines.
The settings of the ultrasound scanners and the contrast dosages are well standardised and make contrast echocardiography an easy to use technique.
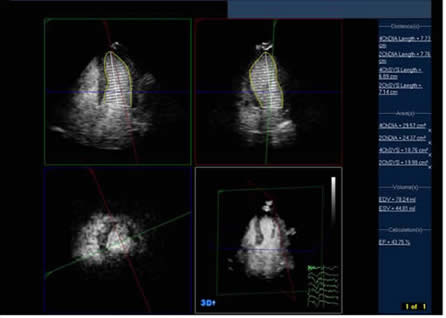
Figure 1 : Improved endocardial delineation following SonoVue infusion: 4, 2 chamber (top left and right), short axis view and multiple plane view bottom right and 3D reconstruction left, obtained from a native real-time contrast 3D dataset. The stress recordings show perfusion defects (arrows). Notice the excellent delineation of the endocardial borders.
There are three aspects, when different imaging technologies are compared: the accuracy, the risk / benefit and the costs / effectiveness (Table 1). Cardiac MRI, CT and nuclear methods are known to be considerably more expensive than contrast echocardiography. Several multicentre, and numerous single centre trials as well as series of case reports have demonstrated the accuracy of contrast echocardiography for assessment of LV volumes and ejection fraction (overview in 6) . The reproducibility of contrast enhanced echocardiography is as good as that of MRI. For assessment of global and regional LV function, controlled large trials are conducted on a large number of patients. The accuracy of stress echocardiography is not worse compared to myocardial scintigraphy. Multi-slice CT is a new technology and a better option to display the coronary arteries compared to myocardial ischemia. There is an ongoing debate whether non-invasive coronary angiography is really providing the best information for the patient management. But there is consensus that functional assessment of coronary stenoses with a stress tests cannot be given up.
Contrast echocardiography could hardly be advocated if there is an imaging technology for the same indication with similar accuracy but a better risk / benefit ratio. There are immediate risks in using contrast agents during MRI, CT and SPECT examinations and long-term risks from the radiation by SPECT and cardiac CT. The latter may become important, if repeated examinations are necessary. For single test, however, the incidence of side effects appears to be very low for all imaging technologies. Therefore, it is difficult to establish a significant superiority of one method over another concerning safety.
In many patients the clinical course requires several appointments for cardiac imaging. Radiation dosages become an issue in patients, who need coronary angiography and coronary interventions. This has to be taken into account, when the patients need functional imaging. MRI and echocardiography should rather be used instead of nuclear methods. Contrast application can close the gap between MRI and echocardiography in those patients with suboptimal images. Moreover, contrast echocardiography remains a very cost-effective test and can be easily integrated into the workflow of an outpatient appointment of the treatment on a ward.
Cost-effectiveness of contrast echocardiography has been demonstrated in patients with difficult acoustic windows.
Appropriate use of contrast for image enhancement is cost-effective because it substantially improves the image quality (and helps to avoid false-positive and negative findings) and favourably impacts the practice of performing additional tests for the same clinical indication. Thanigaraj et. al. estimated savings of US$ 238.00 / patient undergoing contrast enhanced stress echocardiography when baseline images are suboptimal.
This raises the question whether contrast agents should be used in all patients referred for stress echocardiography. However, the use of contrast in all patients who were analysed with a model based on previously published patient outcomes was not cost-effective.
Tardif et. al. demonstrated that contrast echocardiography has a similar success rate compared to nuclear perfusion imaging in diagnosis CAD, but has a 28 per cent (~US$ 170 Can) lower cost and has the potential of additional cost savings through the elimination of further diagnostic tests.
TTE is frequently used in patients who are in ICU to assess LV function. However, if TTE is not possible (or diagnostic) in these patients a time-consuming and expensive TEE is usually needed. Yong et. al. demonstrated that the use of contrast in technically very difficult studies improves visualisation of the ventricular endocardium and increases the accuracy of interpretation of regional and global LV function. Contrast echo was cost-effective compared to TEE in determining regional and global ventricular function, with a cost saving of 3 per cent and 17 per cent, (US$ 43 and US$ 423) respectively.






